
Research Article | DOI: https://doi.org/10.31579/2578-8868/021
1Department of Neurosurgery, Cuba
*Corresponding Author: Carlos Rath,Department of Neurosurgery, Cuba
Citation: Carlos Rath, Jodi Lewis , Neuroinfectious Diseases: Guillain Barre Syndrome Clinical Features Suggestive of Early Diagnosis, Doi: 10.31579/2578-8868/021
Copyright: © 2017 Carlos Rath ,This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 April 2017 | Accepted: 28 April 2017 | Published: 11 May 2017
Keywords: guillain barré syndrome; campylobacter jejuni; antiganglioside antibodies; intravenous immunoglobulin treatment; plasma exchange
Guillain Barré syndrome is one of the best examples of a post infectious immune disease and offers insights into the mechanism of tissue damage in other more common autoimmune diseases. Controlled epidemiological studies have linked it to infection with Campylobacter jejuni in addition to other viruses including cytomegalovirus and Epstein Barr virus. The syndrome includes several pathological subtypes, of which the most common is a multifocal demyelinating disorder of the peripheral nerves in close association with macrophages. Evidence from histological examination of peripheral nerve biopsy and postmortem samples suggests that both cell mediated and humoral mechanisms are involved in the pathogenesis. Immunological studies suggest that at least one third of patients have antibodies against nerve gangliosides, which in some cases also react with constituents of the liposaccharide of C jejuni. In the Miller Fisher variant of the disease, these antiganglioside antibodies have been shown to produce neuromuscular block, and may in part explain the clinical signs of that disorder. Treatment with both intravenous immunoglobulin and plasma exchange reduces the time taken for recovery to occur, although mortality remains around 8%, with about 20% of patients remaining disabled.
The year 2016 marks 100 years since the first description of Guillain–Barré syndrome (GBS), which is now recognised as the commonest cause of acute post-infectious flaccid paralysis worldwide.1 Although rare (with an incidence of 1–2 cases per 100 000), GBS remains an important neurological emergency. The majority of patients with GBS develop ascending paralysis, which starts in the legs and typically spreads to the arms. Cranial nerve involvement is also common and 25% of patients develop respiratory depression and require mechanical ventilation. In Miller Fisher syndrome, which is a rare variant of GBS, cranial nerve involvement and ataxia predominate. Awareness of early symptoms and signs can lead to earlier referral to secondary care, and therefore earlier treatment. In this mini-review we highlight the core clinical features of GBS and discuss important differential diagnoses.
PATHOGENESIS
GBS is a post-infectious neuropathy and known to be triggered by certain infections, including Campylobacter jejuni, Haemophilus influenza, Mycoplasma pneumoniae, Epstein–Barr virus, cytomegalovirus, hepatitis E, and influenza virus.One question patients may ask their GP is: can the flu vaccine trigger GBS? Although this was thought to be a problem in the 1976 swine flu epidemic, recent studies have shown that the flu vaccine does not trigger GBS, and in fact patients who contract influenza virus are at greater risk of developing GBS.
Material & Methods
This study was conducted at Bhopal Memorial Hospital and Research Center (BMHRC), Bhopal, India, after obtaining the ethical approval by the Institutional Ethics Committee. In this retrospective analysis, medical records of 66 referred cases with the diagnosis of GBS admitted to BMHRC from 2002 to 2013 were reviewed and analyzed during April to June, 2014. The data related to age, sex, date of admission, antecedent illness, duration of symptoms before admission, muscle power graded by the Medical Research Council (MRC) scale [ Hughes' functional scores (F-Scores)15, details of Intensive Care Unit (ICU) complications if any, need for ventilation, details of investigations including CSF and electrodiagnostic analysis, complete blood profile, lipid profile, serum electrolytes, coagulation profile, blood grouping and information about TPE as therapy instituted were obtained. As per the hospital policy, all patients received TPE as the treatment of choice. Critical and supportive care comprising respiratory care including mechanical ventilation as and when required, cardiac monitoring, DVT prophylaxis, management of infections, nutritional care and physiotherapy were integral part of the treatment. Patients were classified according to MRC Manual Muscle Testing grading system (0-5) and functional grading scales: grade 0 - healthy, grade 1 - minor symptoms and signs of neuropathy, grade 2 - able to walk five min without assistance, grade 3 - able to walk five min with assistance, grade 4 - confined to bed or chair bound, and grade 5 - requiring assisted ventilation. All patients were divided into four groups based on the four seasons of the year depending on the time of their admission in the hospital. The groups were named as S1 spring season (February to April), S2 summer season (May to July), S3 rainy season (August to October) and S4 winter season (November to January) considering the geographical situation of central India.
Results
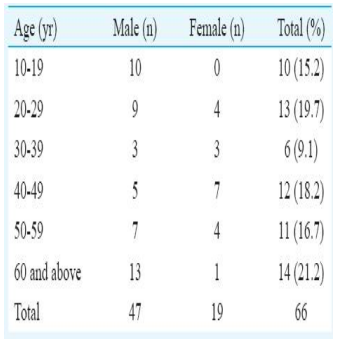
Of the 66 patients, 47 were male. The mean age of the patients was 40.69±18.8 yr. The mean ages of male and female patients were 40.82±21.19 yr (10-74 yr) and 40.36±11.34 yr (20-60 yr), respectively. The male-to-female ratio was 2.4:1. Maximum number of patients (21.2%, n=14) were in the age group of 60 yr and above. The next common age group was 20-29 yr in which 19.7 per cent (n=13) patients were seen [Table 1].
Nearly 62.1 per cent patients (n=41) had history of preceding illness [Table 2].

Flu-like illness as evidenced by fever and cough was found to be the most common antecedent event preceding GBS in 24.2 per cent patients (n=16) followed by gastroenteritis in 13.6 per cent patients (n=9). One patient each presented with the uncommon antecedent events as food poisoning and malarial fever. All patients developed neurological illness within two weeks of the onset of the symptoms [Table 3].
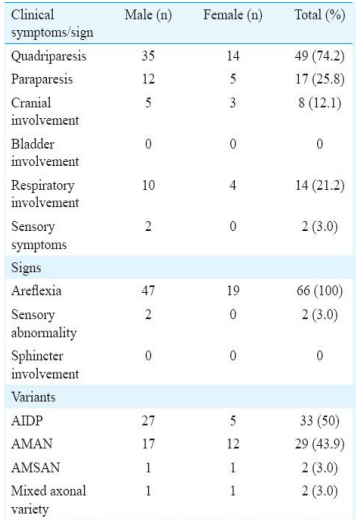
Majority of the patients were admitted to the hospital with progressive weakness in all four limbs (quadriparesis) in 74.2 per cent patients (n=49) as a common clinical feature followed by paraparesis in 25.8 per cent patients (n=17). Dysphagia and respiratory distress were noted in eight patients (12.1%) each. None of the patients were found to have bladder and bowel involvement. All patients had areflexia and two patients (3%) developed sensory involvement All patients underwent nerve conduction velocity testing as the diagnostic testing. The majority (n=33, 50%) were found to be of AIDP followed by AMAN variants (n=29, 43.9%) and 3.0 per cent patients (n=2) were diagnosed as AMSAN.
Discussion
In our study, there was a male preponderance (more than twice that of females) which conformed to the findings of a systematic review which reported that the incidence increased with increase in age, 50 or more years and the distribution of age existed with two peaks In our study, progressive muscular weakness of all four limbs was the common presenting clinical feature and flu-like illness followed by gastroenteritis the most common antecedent illness, similar to that reported earlierThe most common variant of GBS was AIDP followed by AMAN. Other studies from different parts of the world have reported 80-90 per cent frequency from Europe and the USA and Indian studies reporting 48.8 to 85.2 per cent A large study from northern India comprising 328 patients reported AIDP in 73.8 per cent patients and better outcome compared to AMAN . Contrary to our findings, AMAN has been reported at a frequency of 67 per cent in a study from Bangladesh .
In this retrospective analysis, two peaks were found with equal number of GBS patients, one in S1 group (February to April) and the other in S2 group (May to July). Sharma et al [have reported maximum cases in summer (May to July), with majority of patients presenting in the month of May. The seasonal variation may be attributed to the sudden temperature differences in the seasonal conditions making certain months more prone to infections of gastrointestinal and respiratory tract, important antecedent factors of GBS. A study from Southern Iran reported significant seasonal and monthly variation with 50 per cent patients being admitted from February to June and maximum occurrence in spring and winter [. Sriganesh et al[reported a higher incidence between March and August, similar to our study. Zaheer et al]reported a bimodal incidence of GBS during April-May (24%) and July-August (32%) as compared to the other months of the year. Kalita et alhave reported poor prognosis in AMAN variant mostly occurring in summers and complete recovery in AIDP variant which was frequent in rainy season. Our study also demonstrated that in GBS and its variants, respiratory complications (maximum in S4) and duration of hospital stay (maximum in S3) showed a seasonal variation. However, the sample size was small to establish this association clearly and retrospectively limited parameters were studied. About 12.12 per cent patients reported respiratory complications and one patient required mechanical ventilation and scored poor grade on F-score and muscle power grading of 1/5 on MCR scores. Many factors seem to be predictors for respiratory complications and thereby mechanical ventilation including progressively rapid muscular weakness, ineffective cough, bulbar involvement, rapid decrease in vital capacity. Critical care unit is required for the management of GBS patients with respiratory involvement Hughes et al[ reported rehabilitation as important as the immunotherapy and considered it as an integral part of the treatment of the patients with GBS. In our study, proper turning and positioning of patients to prevent bed sores and exercise therapy for maintaining muscle tone and further improvements of power were an important part of multidisciplinary care. None of the patients died during the time of the treatment and only one patient required ventilator support. All patients were advised physiotherapy treatment during the time of discharge. Early detection of the symptoms and early interventions are important factors for better prognosis of GBS
The efficacies of various modalities of treatment in GBS have been a matter of discussion and debate. Hughes et al] reported both TPE and IVIg as equally effective treatment modalities of GBS. Another study reported similar effectiveness of TPE in the treatment of various neurological diseases including GBS In this retrospective analysis, TPE was used as the standard treatment of choice in all seasons. All patients were stable and recovered well and improved in their functional grade and MRC scores at the time of discharge. No mortality related to pulmonary embolism was noted.
In this study, the outcome analysis was limited to the period of hospital stay of the patients. A further study can be designed to assess the outcome analysis of the patients on regular follow up after discharge. Further, climatic conditions might vary from region to region within the country and in other parts of the world making the observations differ. Finally, being a tertiary care centre, patients do not come directly and are referred early for TPE mainly before developing serious complications. Thus, only one of our patients was shifted to ventilator and hence the study analyzed the non-ventilated patients in majority. However, it can serve as an adjunct to other studies done on the ventilated patients. A well-designed prospective analysis needs to be planned to study the effect of seasonal variations in the patients with GBS across the various geographic locations along with markers to establish the associations in terms of clinical features, demographics and type of immunotherapy given.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,

![[Table 1]](http://www.ijmr.org.in/viewimage.asp?img=IndianJMedRes_2017_145_2_203_208371_t3.jpg){kind=link}
![[Table 2]](http://www.ijmr.org.in/viewimage.asp?img=IndianJMedRes_2017_145_2_203_208371_t4.jpg){kind=link}
![[Table 3]](http://www.ijmr.org.in/viewimage.asp?img=IndianJMedRes_2017_145_2_203_208371_t5.jpg){kind=link}